



Electronic health records have been the butt of complaints for years (and in fact, doctors are getting less satisfied with them over time), but we don’t really know how to make them better–if we did, we would have fixed them long ago. Two principles raise the hope of improving the usability of EHRs in the future:
- Involve the clinicians themselves intensively in design.
- Allow access by third parties who can experiment with new innovations.
One specific improvement in user interface design is now being proposed: a better organized display for lab tests. This deserves more news coverage in its own right, and additionally illustrates the two principles at work. I talked recently to Dr. Robert Coli, the chief proponent of the design.
A uniform display format
Current lab results tend to be presented as incomplete and badly fragmented data, instead of the complete, integrated, and actionable information that physicians and patients need. Fragmented data wastes a lot of space, doubles or triples the number of screens to scroll and pages to turn, and lacks the connections that could help physicians draw conclusions. Confusion over test results slows down physicians and increases the risk of errors, both of omission and comission. Doctors might reorder tests merely because they are time-constrained and have trouble finding what they need: the results of recent tests and historical trends.
The proposed user interface adheres to a uniform format developed by doctors, with input and feedback from doctors and nurses to ensure it is clinically intuitive. It will help physicians as well as patients view and share test results displayed by EHR, PHR, and HIE platforms. A group of Rhode Island physicians have supported its development and unsuccessful efforts to distribute it as a commercial product for more than 20 years. Various levels of display are illustrated on their web page.
Their key advance, based on principles of human-centered design, is to group tests by organ systems (a classification that already exists in medicine) and then to display them chronologically within clinically logical categories and subcategories. In one example, the first three subcategories of the first main test category, “MICROCHEM TESTS,” displays about 50 clinical lab tests that are most frequently ordered and repeated. The less commonly ordered and less frequently repeated lab tests are displayed in the fourth subcategory, with Microbiology results presented in subcategory five. Clicking on rows will display useful details, including reference ranges and units.
In the second main test category, “SUBSPECIALTY TESTS,” imaging, endoscopic and other testing modalities are indexed by organ system and clinical specialty in alignment with physicians’ common thought flow and workflow.
According to Coli, existing displays are packed with fragmented data. They use five times as much space, are more confusing, and make it difficult to find individual test results or to follow trends over time. The same flawed user interface design seems to have persisted for an astonishingly long time. Figure 1 shows a printed hospital report of lab results dating from the 1970s, while Figure 2 shows a modern EHR display using the same suboptimal design. Both reporting formats list tests in a rather haphazard order over short time periods, include an enormous amount of useless white space, and are laid out inconsistently to that doctors cannot find important information quickly even after considerable practice.
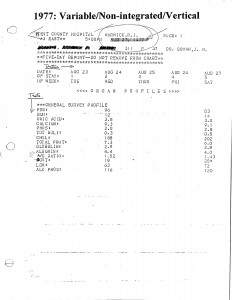
Figure 1. Old paper lab results report
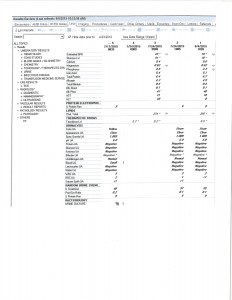
Figure 2. Putatively modern electronic display of lab results
Often, user interface advocates call for customizable interfaces. But Coli argues that for lab and other test results, consistency is generally more important than customizability. A single, platform-neutral, uniform report display will allow doctors to quickly learn how to find the information they are seeking and apply these skills throughout their careers, at any point of care. The format could also be the basis for other enhancements, such as showing a chart with a normal range and the patient’s actual result, and using color to highlight anomalies. Specialty-specific customized views of cumulative results and Clinical Decision Support (CDS) applications for optimizing cost-effective test selection can also be developed as value-added enhancements to the standard reporting format.
History of the proposal
Coli rebelled at lab test displays back in the days of paper, and developed his current format when starting his own practice in 1979. Enthusiasm grew among his colleagues, but he could not drive adoption outside the circles of clinicians who knew and respected him. Amazingly, he has kept up his efforts over the years, and saw the passage of HITECH as the opening he needed.
Between 2011 and 2013, Coli accepted an invitation from Direct Project Coordinator, Arien Malec, to attend weekly virtual meetings of the Standards & Interoperability (S&I) Framework as it developed HL7-balloted implementation guides, pilot projects, and reference implementations for key lab-related standards. Although the Framework’s scope of work did not include standardizing the presentation of test results for physicians and patients, it was relevant to other Framework efforts, including EHR-LIS open source lab results reporting, lab test ordering, and an electronic directory of lab services standards. Coli’s proposal also drew approval from the judges of the eHealth Initiative’s 2015 Innovation Challenge.
Coli is currently investigating possible work with the Healthcare Services Platform Consortium (HSPC) to implement the standard reporting format over SMART on FHIR. And he’s in the process of connecting with all the right consortia actively seeking to advance interoperability, including the CommonWell Health Alliance and the Argonaut and Sequoia projects. Recognizing the spread of open source solutions in health care, Coli is offering these public/private sector consortia and leading standards organizations a royalty-free license to a patent that his company holds on the format.
Still, vendors have taken little notice of the lab results format. This is why a third-party market is so important. There is no reason for suffering clinicians to wait until one implementation detail rises high enough on some vendor’s checklist to have it done. Tools and standards have advanced to the point where innovations like this can be developed and disseminated quickly.







